|

|
  |
by Sherry Baker
The landscape wasn't the only surprise Witte would find during the next three months. In Kenya, she became immersed in a culture faced with public health problems she had only known from afar. These public health concerns loomed large in a land where 2 0% of the children die before the age of five. Witte had come to Kenya to assist in a collaborative public health program between CDC, the CDC Foundation, and CARE. Funded by the Robert W. Woodruff Foundation, it is an effort to help villagers improve their own health care. Health care professional s from CARE train health care supervisors from the area in diagnosing, preventing, and managing the major childhood killers in Kenya - diarrhea, malaria, and respiratory infections. The supervisors, in turn, train volunteer health care workers elected by residents of each of the eight to ten villages under their watch. CDC researchers work collaboratively with CARE to evaluate the project and target interventions that can provide faster access to appropriate health care for seriously ill children. Witte, with an undergraduate degree in Russian, developed an interest in international public health issues while working in CDC's Office of Global Health in 1996 and 1997. As a visiting fellow, she helped coordinate a child survival project in the Cen tral Asian Republics of the former Soviet Union. Instead of taking a vacation last summer, Witte decided to look for a job that would involve field experience, which led her to the project in Kenya. The summer in Kenya helped prepare Witte for her second year of medical studies that are now drawing to a close. The children she saw in Africa were dying of the same infectious and parasitic diseases, such as malaria and pneumonia, that her sophomore medical training covered. Witte believes the Kenyan experience served as a valuable precursor to her studies at the Rollins School of Public Health, which she will pursue after her third year of medical training. "I think it's important to see your individual patients in a broader context, and public health helps you do that," Witte says. "It helps you understand why particular people have particular diseases and to seek possibilities for preventing those disea ses. I saw these concepts in action in Kenya." |
 n her way to Siaya, Kenya, last summer, Janet Witte thought she'd find a lush tropical setting. Instead, the rolling land was parched. "It was the dry season," recalls Witte, a joint degree student at the Rol
lins School of Public Health and Emory School of Medicine. "Everything was dusty and barren. A 'crop' of corn, kale or beans sometimes consisted of a few straggly plants."
n her way to Siaya, Kenya, last summer, Janet Witte thought she'd find a lush tropical setting. Instead, the rolling land was parched. "It was the dry season," recalls Witte, a joint degree student at the Rol
lins School of Public Health and Emory School of Medicine. "Everything was dusty and barren. A 'crop' of corn, kale or beans sometimes consisted of a few straggly plants."
  |
 itte accompanied health care workers to rural homesteads, comprised of extended families living in groups of mud huts. She helped collect data from primary caretakers, usually mothers. She asked about the sy
mptoms of children who had died, what treatment they had received, and how long they were sick before help was sought. "We also asked what they thought caused the disease, what they thought could have prevented it, and what the symptoms of the final disea
se were - which allowed us to target the likely cause of death," Witte says. itte accompanied health care workers to rural homesteads, comprised of extended families living in groups of mud huts. She helped collect data from primary caretakers, usually mothers. She asked about the sy
mptoms of children who had died, what treatment they had received, and how long they were sick before help was sought. "We also asked what they thought caused the disease, what they thought could have prevented it, and what the symptoms of the final disea
se were - which allowed us to target the likely cause of death," Witte says.
As she collected information from questionnaires, interviews, and death certificates, Witte was often overwhelmed by the tragedies she encountered. She recalls a visit to one homestead where she saw the mud huts typical of a Kenyan village. Yet, someth ing seemed odd. "Usually, there were preschoolers running around, playing," she says. "Suddenly, I realized there were no children. They had all died." One woman she interviewed had lost all six of her children to disease. Another woman had returned to her village after living in an urban environment. One of her children had died, and her remaining child was not growing properly. During the interview, Witte says, the woman explained she was a guest in the homestead and n ot high in the village hierarchy, so her child received little food. "The extension worker told her she needed to fight for her child, to get her enough food so she would grow and get well," Witte says. "She explained how to combine locally grown foods to provide adequate nutrition for the child. The woman was obviously receptive to this knowledge and support." In another homestead, Witte vividly remembers a tiny, four-year-old girl: "Both her parents had died. She was living with her elderly grandmother, who was clearly overwhelmed. Yet this little child, wearing a tattered dress, was washing a huge stack of dishes, happily singing the entire time. I wondered if she would live to be five." In fact, Witte says, in every homestead, at every interview, she would look at the surviving children and wonder: Who will make it? Which child will die? "And you have to question what this does to the bond between mother and child. Do mothers cherish the children more because they may die? Or is it harder to become attached to your child if you know you may lose him?" |
 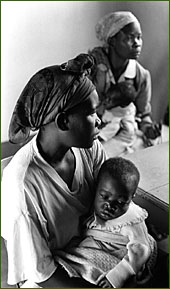 Witte helped collect data from mothers of children who had recently died, asking what treatments the child had received and how long the child was sick before help was sought. The interviewers also asked the mothers what they thought had caused the disease and if they had ideas about what could have prevented it. |
itte is optimistic that public health interventions in Kenya will eventually lower the childhood death rate substantially. But she knows there is no easy fix: "Health care workers can sell mosquito nets at c
ost, but if the husband thinks it's a status symbol and insists on sleeping under it, instead of the children, the kids will still get malaria," she says. "Spiritual beliefs about causes of deaths - like a look from 'an evil eye' - are deeply ingrained. T
hose beliefs lead mothers to seek help for their children from traditional healers rather than medical dispensaries or CARE volunteers."
Before leaving Kenya, Witte visited a traditional healer herself. After paying the elderly man, Witte was shown the tools of his trade - rocks, herbs, a cow horn. "He handed me a stone, had me put it in the horn, and said to think of a problem I needed to have solved. He held the horn upside down and the rock fell out. We repeated the process several times, but when it finally remained stuck, he said the ancestors had accepted my problem and would try and help." Witte found the experience therapeutic. "I told him my problem was getting back to America safely. He looked me straight in the eye and said he understood, we had talked to the ancestors, and I would have a good journey back. It made me feel good. I co uld see that the traditional healer does have a valid role in the healing process - but, obviously, he can't do everything." "It is counterproductive to challenge the mothers' traditional beliefs," Witte says. "It is far better to explain that traditional healing has its place, but when a child has specific danger signs of disease, they need to immediately go to a qualified caregiver who can give out effective medicine. As more children visit the community health workers and are cured by the treatments offered, in time I think more people will understand that those treatments work." Although she has a strong interest in both pediatrics and psychiatry, Witte hasn't decided what specialty she'll pursue in her medical career. "But work that combines clinical practice and public health would be ideal," she says. "I'm especially intere sted in the relationship between medicine, society, and health - particularly mental health. I think mental health epidemiology will be an important area of research in the future." Last summer, Witte lived in a hotel with no running water, no oven for the chef to cook food, and the only phone in town. Now, settled back into her life as an Emory student, Witte is far removed from her sojourn to Kenya - but not its impact. "It gave me hands on experience. I learned first-hand about a grass roots community project. And I came away from the experience committed to continuing my education. Also, I have a new understanding about why it is so important to rigorously evaluate public heal th programs and find out what really works."
|
Spring 1999 Issue | Dean's Message | Risky Business | All the Pretty Poisons | Season of Change
WHSC | RSPH
Copyright © Emory University, 1999. All Rights Reserved.
Send comments to hsnews@emory.edu.
Web version by Jaime Henriquez.