
|
 |
 |
On November 12, 1996, an audience gathered in Cannon Chapel on the Emory campus to hear Public Health Dean James Curran lecture on AIDS. Part of the university's Great Teachers Lecture Series, this was Curran's third time to speak about the epidemic in a church setting, having previously discussed AIDS in a synagogue and at the Convent Avenue Baptist Church in Harlem. During the hour-long lecture in Cannon Chapel, Curran brought the audience news suited to be heard in church--news about the history of a disease that demands reverent ears for hearing, news that for the first time may offer some bit of hope. One of a handful of scientists to encounter AIDS before it even had a name, Curran is an undisputed expert on the AIDS epidemic. At the Centers for Disease Control and Prevention (CDC), he headed the Task Force to investigate the first reported cases i n 1981. Subsequently he directed the Division of HIV/AIDS in 1989 and was appointed assistant surgeon general of the United States in 1991. He continues to serve as an adviser to both the Combined United Nations Programme on AIDS and the National Institut es of Health on HIV, and as a member of the board of the National AIDS Fund. Locally, he serves on the board of AID Atlanta and the scientific advisory board of Jerusalem House. When Curran left the CDC to accept the position of dean in 1995, President Bill Clinton sent thanks for Curran's work: "Your leadership in the area of HIV and AIDS prevention strengthened our global response to this epidemic and served as a calm voice of scientific reason during some difficult times." This night in Cannon Chapel, Curran shared that calm voice and his firsthand understanding of a disease that has reshaped our world. |
  |
AIDS is a new disease. It seems hard to believe, but it didn't exist at all until a few decades ago. We now live in a different world because of a single infection. I am part of the last generation to go through its first sexual experiences with out the fear of AIDS. My kids are part of the first generation to grow up with AIDS. For countless billions of people, life has changed because of this new disease. In June of 1981, the first cases of Pneumocystis pneumonia were reported. At the CDC, I was assigned to a task force to study these cases. We thought we'd work on it for three months. We could not readily comprehend we were at the beginning of an era. The years from 1981 to 1986 were the era of discovery in AIDS. Scientists made mind-boggling discoveries. The fatal opportunistic infections and cases of a rare cancer were confirmed consecutively in homosexual men, persons who injected drugs, and thei r sexual partners. But it was the documentation of unexplained Pneumocystis pneumonia in three men with hemophilia that proved the syndrome of acquired immunodeficiency was caused by an agent transmissible in blood. Men with severe hemophilia lack necessary factors to cause blood to clot following bleeding. In the 1970s and early 1980s, this disorder was treated with concentrated clotting factor, pooled from the plasma of thousands of individual donors. Since the average person with severe hemophilia was thus exposed to hundreds of thousands of donors, this group logically was the first to show signs of transfusion-associated AIDS. The hemophilia cases helped scientists prove that AIDS was caused by a virus and ga ve them a place to look - in the blood. The virus that causes AIDS, HIV, was discovered in 1983 by investigators at the Institute Pasteur. Shortly thereafter, tests to detect the presence of the virus in blood demonstrated that hundreds of thousands of Americans had already been exposed and remained infected. Although only several hundred had developed AIDS at that time, epidemiology studies revealed that the infections appeared to inevitably progress with time. Four years after the first cases were detected, the vast extent of the epidemic was becoming horrifying clear. We then knew that hundreds of thousands of Americans had a progressive illness and would likely die of AIDS during the next decade. |
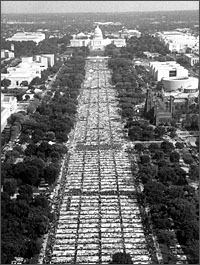
  The AIDS Memorial Quilt, composed of 40,001 3-foot by 6-foot panels, has been shown in thousands of locations, including Emory University. Each panel commemorates the life of someone who has died of AIDS complications, with 12% of all US AIDS deaths being represented. |
The recognition of the extent of the AIDS epidemic and its transmissibility through sexual contact and blood transfusion had an enormous impact on society. Fear led to discrimination. During the period of growth from 1986 to 1991, for example, R yan White was kicked out of school because of the community's fear. The government ran ads during this era to educate the public with slogans like "You Won't Get AIDS From a Bug Bite." As the number of AIDS cases grew so did government expenditures and the number of health and social service workers and volunteers to combat the problem. With so many individuals working together, there was a sense of optimism that the pace of scientif ic discovery assured both a vaccine and a cure. Ironically, few scientific discoveries were announced during this period. But the discoveries of the 1990s, including the development and testing of protease inhibitors and the successful prevention of perin atal transmission, had their origins in the scientific foundation laid during the era of growth. By 1991, the number of new cases had begun to level off in the United States, and much of the country became complacent about AIDS. |
  Placed side by side, the panels of the AIDS Memorial Quilt - sewn by family, lovers, and friends of those who have died of AIDS complications - fill the surface of 15 football fields. Photographs by Paul Margolies, courtesy of the Names P roject Foundation. |
In 1992, we entered the current era, which will undoubtedly be a long haul. The rates of AIDS in this country are two to eight times larger than in other industrialized nations. Since 1992, HIV has been the leading cause of death in the age grou p from 25 to 44, accounting for one out of every five US deaths. In the world, more than 30 million people are infected. The epidemic is rampant in South America, exploding in many countries in Southeast Asia, and has become an ultra-epidemic in Africa. H IV is the leading cause among all deaths in many African nations. We have had some prevention successes. Even before the discovery of HIV, the CDC provided solid recommendations for prevention based on epidemiological findings. There was a dramatic change in sexual behavior in gay men and an actual decline in HIV tra nsmission in this group by the mid to late 1980s. Today blood is far safer than it has ever been, and the risk of acquiring HIV through transfusions in the United States is virtually nil. Recently, there have been reports of declines of HIV in adolescent women in Uganda, where prevention activities have been extensive and received community-wide support. In Thailand, which spends more money per capita on HIV prevention than we do in the United States, HIV incidence has declined substantially. A study supported by the National Institutes of Health among pregnant women infected with HIV has shown that AZT given during pregnancy, delivery, and to newborns for six weeks after birth leads to a 66% reduction in HIV transmission to the newborn. Following these findings, routine counseling and voluntary HIV testing has been recommended for all pregnant women in the United States, and HIV transmission has declined dramatically in the United Stat es. The new class of drugs called protease inhibitors used in combination therapy brings many people from their death beds back to healthy and productive lives. Though the long-term effectiveness of these therapies will take several years to assess, the sh ort-term results are promising. Providing these drugs to all Americans in need will be an economic challenge. The cost of HIV care remains out of reach for most infected persons. |
 |
Barriers to HIV prevention include denial, discrimination, and scarcity of resources. The first factor that contributes to denial is the long time between when people are infected with the virus and when they actually get sick. Ignorance about o ne's own risks feeds denial, especially among teenagers and young adults. Like weeds in a garden, discrimination keeps coming back, whether it is based on gender, race, sexual orientation, or HIV infection status. Many people with HIV or at increased risk for the virus fear discrimination, sometimes to the extent that they a void HIV testing or care. Perhaps the greatest barrier to prevention is scarcity. Competition for health care and research resources will become even greater during the next decade. Prevention and education services, especially for the poor, will be stretched as well. |
 |
Solutions to HIV prevention and care will require commitment and leadership. This leadership consists of reaching consensus on a common goal and rising above our differences. HIV is a formidable foe and a horrible disease, but the infection is pr eventable. Together we can conquer it. |
Spring 1997 Issue | Our Modern Plague | A Prayer for AIDS | REAL Life Lessons
Putting a Price on Prevention | An Epidemic Ignored | It's MAGIC | Supporting Player
School Sampler | Alumni Sampler
WHSC | RSPH
Copyright © Emory University, 1998. All Rights Reserved.
Send comments to
hsnews@emory.edu.
Web version by Jaime Henriquez.