 | 
|
by Jeanie Davis
"The effect of AIDS has been devastating for black people," says Robinson. "It has destroyed many individuals, families, and communities. If we in the church don't begin to educate our people about it, if we don't stop the stigma, we're going to be los t." It is a time of crisis in the African-American community, says Stephen B. Thomas, associate professor at the Rollins School of Public Health. "At a time when new AIDS cases are declining for whites and new drug therapy is extending life, blacks are dyi ng of AIDS at an alarming rate." The overrepresentation of African-Americans among AIDS cases has been well documented through the first decade of the disease. Blacks constitute 12% of the US population, yet they represent 34% of all AIDS cases in the United States. Among all women wi th AIDS, 57% are black. Among all children with AIDS, 58% are black. The disproportionate spread of HIV in the African-American community is expected to continue throughout the second decade of AIDS. |
 Pastor Julia Robinson |
 t is Saturday morning, and Sabbath services are under way in a small, weathered chapel just outside of Atlanta. Welcome to Believe and Receive Ministries. From the pulpit, Pastor Julia Robinson is delivering
a sermon about compassion for those who live with AIDS. The topic would scare other ministers. But Robinson believes in erasing the stigma associated with AIDS in her community. In the past year alone, she has spoken at more than 40 churches and schools,
presenting scientific facts that debunk myths about the epidemic. In the three years since the founding of her church, the reputation of her AIDS ministry has spread throughout Atlanta's black community.
t is Saturday morning, and Sabbath services are under way in a small, weathered chapel just outside of Atlanta. Welcome to Believe and Receive Ministries. From the pulpit, Pastor Julia Robinson is delivering
a sermon about compassion for those who live with AIDS. The topic would scare other ministers. But Robinson believes in erasing the stigma associated with AIDS in her community. In the past year alone, she has spoken at more than 40 churches and schools,
presenting scientific facts that debunk myths about the epidemic. In the three years since the founding of her church, the reputation of her AIDS ministry has spread throughout Atlanta's black community.
 or more than ten years, Thomas has worked to raise awareness about HIV/AIDS as well as to understand why so many
African-Americans hesitate to follow public health advisories. or more than ten years, Thomas has worked to raise awareness about HIV/AIDS as well as to understand why so many
African-Americans hesitate to follow public health advisories.
The problem of "excess deaths" in minority populations first caught his attention during graduate school days in the 1980s, when he read a government document, "The Secretary's Task Force Report on Black and Minority Health." The report described the s tate of health in the American population. Commissioned by the Secretary of Health and Human Services, the report described high death rates among black populations due to preventable risk factors for cancer, cardiovascular disease, diabetes, violence, an d substance abuse. Among blacks, the report described "excess deaths" from these diseases. "That report really guided my work toward minority health," Thomas says. In 1985, when he joined the faculty at University of Maryland, Thomas began building bridges into the underserved segments of the Baltimore and Washington, DC, communities--and figuring out how to prevent disease and promote health in the black communi ty. By then, AIDS was emerging as a worldwide epidemic. Thomas designed and taught the university's first course on AIDS education and prevention. When the CDC launched the first federally funded program directed to community-based organizations serving minority populations in 1987, Thomas designed a program called RACE (Reducing AIDS through Community Education). He then monitored its success. T he program showed great promise, because it combined the resources of black churches in five cities with the strengths of a historically significant civil rights organization, the Southern Christian Leadership Conference (SCLC). "It was extremely important for trusted organizations like SCLC to deliver AIDS prevention information to the black community," Thomas says. "It was a way to remove AIDS from the arena of blame and prejudice and put it in the area of civil rights." A national survey sponsored by the SCLC also uncovered unsettling feelings that previously had gone unrecognized. When more than 1,000 educated black church members were surveyed on their knowledge and attitude about AIDS, Thomas and his research collaborator, Sandra Quinn, found that 35% of the respondents believed that the disease was a form of genocide, while another 30% were unsure. If educated African-Am ericans had such feelings, Thomas and others asked, how does that affect their attitudes and behaviors toward the public health system? |
 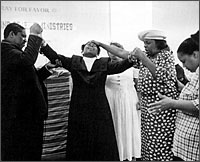 Through Believe and Receive Ministries, Pastor Robinson works to reduce the stigma associated with AIDS in Atlanta's black community. The church is a natural conduit for HIV education programs in African-American communities, according to Associate Professor Stephen Thomas, who advises public health educators to work with church leaders in designing outreach programs. |
 oday, as a tenured associate professor in the Rollins School of Public Health and director of the Institute for Minority Health Research, Thomas is still trying to answer that question. While death rates fro
m AIDS have begun to decline in the white population, African-Americans are still in crisis, he says. And they are refusing to participate in clinical trials of AIDS drugs and HIV vaccines. Why? Thomas wants to know. oday, as a tenured associate professor in the Rollins School of Public Health and director of the Institute for Minority Health Research, Thomas is still trying to answer that question. While death rates fro
m AIDS have begun to decline in the white population, African-Americans are still in crisis, he says. And they are refusing to participate in clinical trials of AIDS drugs and HIV vaccines. Why? Thomas wants to know.
To understand any epidemic's propagation and society's response, we must understand the social context of the population it penetrates, Thomas says. During the past eight years, he has documented reports in the popular black media as well as anecdotal reports from community-based organizations, finding fear, distrust, and suspicion of the medical and public health system in the African-American community. Part of that distrust arises from historic tragedies such as the Tuskegee syphilis study, Thomas says. Begun in 1932, the study examined the effects of untreated syphilis on 412 black men in Tuskegee, Alabama. Many years later, the public health resear chers who ran the study decided to withhold penicillin from the study's participants when it became available as an effective treatment for the disease. Although the efficacy of penicillin treatment at this stage of the disease was not known, many black m en who may have been cured instead suffered and died for the sake of the research, which continued until 1972. "Almost 70 years after that study began and 25 years after it ended," says Thomas, "there remains to this day a legacy of distrust and suspicion that hampers medical research and public health efforts among African-Americans." These perspectives have repercussions for AIDS prevention and treatment, Thomas says. "They are legitimate psychosocial issues that cannot be ignored by health care professionals." Thomas and his research team hope to bring this understanding to a wider audience through events such as one coordinated in February by the School of Public Health, the Ethics Center, and the historically black colleges and universities that make up th e Atlanta University Center. After the Atlanta premiere of Miss Evers's Boys, an HBO original film based on the Tuskegee study, a distinguished panel and an audience of 400 addressed African-American's mistrust of medical research and health delivery systems. Panelists - including CDC Director David Satcher, Morehouse School of Medicine President Louis Sullivan, and Dean James Curran, among others - also discussed the implications of mistrust for the inclusion of African-Americans in research studies. "When the Tuskegee study arises as a justification for fear, we must share the facts and admit to the limitations of science," Thomas says. "Simply to say that nothing like Tuskegee could ever happen again is not enough." In this context, the black church can play a crucial role in combating the AIDS crisis, he adds. |
  James Nolton (left) participates in a recent gathering at Our Common Welfare, a community-based substance abuse program tha boasts higher than normal success rates. Primarily federally funded, the program provides housing, some financial support, and a safety net for its participants. Thomas, who has been studying the program, proposes it as a model for future public health efforts. |
 any black church leaders oppose condom and clean needle distributions. According to Thomas, they want comprehensive health education and drug treatment programs for their congregations, rather than needles,
which they see as perpetuating the drug problem. any black church leaders oppose condom and clean needle distributions. According to Thomas, they want comprehensive health education and drug treatment programs for their congregations, rather than needles,
which they see as perpetuating the drug problem.
"Public health educators could accomplish more by collaborating with church leaders when they create community outreach programs," Thomas says. According to his research, published in The American Journal of Public Health, more than 60% of 635 African-American churches he surveyed collaborate with health departments and other organizations to sponsor community outreach programs, which provide a variety of educational services on topics from human sexuality to drug abuse. "We don't need churches to hand out condoms or to pass out clean needles," Thomas says. "We need churches to reduce the stigma of AIDS." The many denominations of the black church traditionally have addressed the social and health needs of their people. As such, the church has the trust and infrastructure necessary to serve as an effective conduit for HIV education programs, Thomas adds . "The church has always been our support," agrees Robinson. "Even in the days before the civil rights movement, the church always took care of its own. We trust the church." Although many clergy continue to be uncomfortable discussing AIDS, change may be coming from advocacy by people such as Thomas and Robinson. In 1994, for example, Reverend Henry Lyons, president of the National Baptist Convention USA, called upon the " nation's largest black church organization to be a leader in the battles against AIDS." "By working through the black churches, public health educators can influence so cial norms and reach a more general population," says Thomas. "We can dispel many of the myths, lessen the discrimination against those who are at risk or infected, increase public knowledge and support for prevention programs, and ultimately increase sup port of low-risk behaviors." |
  At Our Common Welfare, they call her Mom. Faye Brown-Sperling is the founder and director of the program that strives to make participants drug-free and to return dignity to people affected by HIV. |
|
he Black Church Week of Prayer for the Healing of AIDS has emerged as a way to bring clergy, their congregations, and people affected by AIDS together to discuss a tough issue, says Thomas. The idea evolved
from an annual Harlem Week of Prayer, created nine years ago by Pernessa Seele, a young woman who had lost many friends and family to the disease and in response founded the Balm in Gilead, Inc.
Thomas is conducting research on the Black Church Week of Prayer in six US cities, including Atlanta. With a three-year CDC grant, Thomas is evaluating the Black Church Week of Prayer to determine its effectiveness as a model to tap the church's capaci ty to change attitudes about HIV and AIDS. Robinson organized Atlanta's observance of the event in 1996, bringing black clergy together in round-table discussion groups and prayer sessions. She helped organize special sessions for potential AIDS ministry volunteers, AIDS-infected individuals, f amilies and friends, and teenagers. Community response far exceeded her expectations. "We thought maybe 100 or 200 people would attend," says Robinson. "We got 1,000." She is in charge of the 1997 effort in Atlanta as well . "There are many forms of healing," Robinson says. "Healing can mean there's not another trace of AIDS in your body. It can also mean accepting where you are--and deciding that you can live with the virus." |
 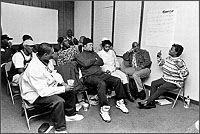 Nearly all the participants at Our Common Welfare are African-American. Many are gay. All have been drug abusers and have tested positive for HIV or have AIDS. |
 ut what about those on the fringes of society, whom organized religion fails to reach? For them, community-based programs like "Our Common Welfare" may be the answer, says Thomas. ut what about those on the fringes of society, whom organized religion fails to reach? For them, community-based programs like "Our Common Welfare" may be the answer, says Thomas.
While most substance abuse treatment programs report that only two out of every ten participants remain drug-free for more than one year, Our Common Welfare boasts a higher success rate. Of the 600 men and women treated there, six out of every ten stay clean. Thomas, who has been studying the program, proposes it as a model for future public health efforts. On the east side of Atlanta, a small suite of offices houses Our Common Welfare, where support groups meet regularly. Nearly all who attend these sessions are African-American. Many are gay. All have been drug abusers and have tested positive for HIV o r have AIDS. "Let's face it, these people are socially unacceptable," says Faye Brown-Sperling, the founder and executive director of Our Common Welfare. "By the time they get here, they've burned their bridges. They've gotten all the financial assistance they can get from any other AIDS service organizations." Family and friends? Forget it, says Brown-Sterling. "Nobody wants them around because of things they've done in the past," she says. "They have HIV, so people are scared of them. My goal is to help these peo ple have some dignity in their lives." Johnny Smith is a favorite example of the program's possibilities. A gay man and a drug abuser, he tested positive for HIV 12 years ago. When Brown-Sperling met him five years ago, he was "sick and tired of being sick and tired," he says. Our Common We lfare was in its infancy, operating out of Brown-Sperling's living room. First, she helped Smith quit using drugs with the Alcoholics Anonymous 12-step program. He eventually became a staff member at Our Common Welfare, counseling other men like himself. "Smith is a mentor for new people that come here," says Brown-Sperling. "They come in and they're scared to death. They think they've got two years to live. He helps them see that there's hope." Using addiction as an ally, Brown-Sperling says, is the secret to her program's success. "Addicts will do anything to get what they want. We teach everyone that they need to have a dream. There's got to be something stronger than addiction that will mo tivate them to action." Her program (primarily federally funded) also provides housing, some financial support, and "the safety net they need," says Brown-Sperling. "I don't know how many people have me as their next of kin on their medical records. They don't have anybody el se. They call me mom." The black church will soon have a presence here as well, with Robinson joining the support groups. Brown-Sperling understands why religion should be part of her program. "If we haven't had anything, black people have had God," she says. "I pray all the time. Sometimes that's all I can do. Whether you call for Jehovah or Jesus or Allah, I know there's something bigger than we are." "There is one thing we know for sure about the experience of black people in America," Thomas says. "They know how to draw upon an endless reservoir of love and hope in the face of adversity." The African-American faith community is a wellspring for th at reservoir and a partner public health educators can trust. |
  A gay man and a former drug abuser, John Smith not only beat his addiction at Our Common Welfare but also joined the staff as a counselor to other men like himself. 
Thomas, director of the Institute for Minority Health Research, wants to improve public health education efforts among blacks. |
Spring 1997 Issue | Our Modern Plague | A Prayer for AIDS | REAL Life Lessons
Putting a Price on Prevention | An Epidemic Ignored | It's MAGIC | Supporting Player
School Sampler | Alumni Sampler
WHSC | RSPH
Copyright © Emory University, 1998. All Rights Reserved.
Send comments to
hsnews@emory.edu.
Web version by Jaime Henriquez.