 |

|
|
Dr. Salk's findings heralded an era of progress in vaccination research. Over the next decade, scientists introduced vaccines to control a host of debilitating diseases. However, as researchers discovered antibiotics, introducing more and more of the w onder drugs to control disease, interest in vaccine studies slackened. "In the 1960s and 1970s, the scientific community believed that the situation in infectious diseases was under control because the vaccines and antibiotics seemed to work so well," say s Elizabeth Halloran, associate professor of biostatistics at the Rollins School of Public Health. According to Dr. Halloran, development of statistical methods for evaluating vaccines in the field did not keep up with methods developed in recent decades to study diseases such as cancer and heart disease. "The measles vaccine, for example, worked so well at the beginning," she says, "that the scientists of the time did not believe they needed fancy statistical methods to evaluate them." Today, however, that situation has changed with the return of new strains of infectious diseases and more powerful strains of diseases previously thought to be controllable. In Bangladesh, a new strain of cholera, known as cholera Bengal, is sweeping t hrough the densely populated country, causing a massive epidemic. In India in 1994, a form of plague resurfaced, sending panic throughout that nation. And worldwide, HIV has infected millions, baffling researchers and eluding vaccination, treatments, and cures. Although thousands of public health workers are currently involved in vaccine research trials throughout the world, only a small number of scientists develop the research design and analytic models essential to those trials. In the Department of Biosta tistics at the School of Public Health, three faculty members belong to that elite group: Drs. Halloran, Michael Haber, and Ira Longini. These researchers develop and apply complex statistical and mathematical models to estimate vaccine efficacy as well a s examine other questions associated with vaccines. They tackle many issues that relate to vaccine efficacy, from how much protection a vaccine affords to an individual to how much a population is protected by a vaccination effort. Although they have different specific interests within the general study of vaccine efficacy, they bring to their work a common interest in combining dynamic modeling and statistical methods of evaluation. With a grant from the National Institutes of Health (NIH), they are collaborating on the development of new methods for e valuating vaccine efficacy. |
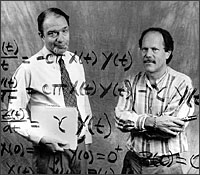 Evaluating efficacy: Biostatistics researchers Michael Haber (left) and Ira Longini develop and apply complex statistical and mathematical models to estimate the efficacy of vaccines for a variety of infectious diseases, from smallpox to cholera to the AIDS virus. |
 n 1952, Dr. Jonas Salk began conducting the field trials of a new vaccine that would halt one of the worst epidemics of poliomyelitis ever in US history. In the laboratory, Dr. Salk had demonstrated that kill
ed virus from three separate strains of the disease could induce antibody formations in monkeys without producing polio itself. The 1952 trials, conducted on children who had recovered from polio and on those who had not had the disease, were a success. I
n 1954, a mass field trial produced further confirmation, and the vaccine became one of a group of required vaccinations for all children in the United States.
n 1952, Dr. Jonas Salk began conducting the field trials of a new vaccine that would halt one of the worst epidemics of poliomyelitis ever in US history. In the laboratory, Dr. Salk had demonstrated that kill
ed virus from three separate strains of the disease could induce antibody formations in monkeys without producing polio itself. The 1952 trials, conducted on children who had recovered from polio and on those who had not had the disease, were a success. I
n 1954, a mass field trial produced further confirmation, and the vaccine became one of a group of required vaccinations for all children in the United States.
 r. Longini gives a straightforward explanation of what the researchers do: "Say you are running an HIV vaccine trial for a year. You have a high-risk population in which all the subjects have been exposed to
the virus. To half of the group, you inject vaccine. To the other half, you give a placebo shot. If 1% of the vaccinated group become infected and 2% of the placebo group develop infection, then you have a 50% efficacy." r. Longini gives a straightforward explanation of what the researchers do: "Say you are running an HIV vaccine trial for a year. You have a high-risk population in which all the subjects have been exposed to
the virus. To half of the group, you inject vaccine. To the other half, you give a placebo shot. If 1% of the vaccinated group become infected and 2% of the placebo group develop infection, then you have a 50% efficacy."
However, that oversimplified explanation, Dr. Longini is quick to add, does not take into account when the subjects were initially exposed to the virus, how often they were exposed, if their behavior changed after receiving the vaccine, and if they tra nsmitted the infection to others. Those factors and others influence the rate of efficacy. Dr. Haber offers another way to think about vaccine efficacy. "Suppose you have just been vaccinated against an infectious disease," he says. "You are told that the efficacy of the vaccine is 95%. You might inquire whether this means that the vaccine r educes by 95% the chances of contracting the disease every time you are exposed, or whether you have a 5% chance that the vaccine has no effect. The difference may not sound very important if your exposure is very rare, and you cannot do much to avoid exp osure. "On the other hand, if the disease is transmitted via sexual contacts, knowing how the vaccine protects you could affect your behavior. In the first case, if you have frequent contacts with infected persons you are still likely to eventually contract t he disease despite the vaccination. In the second case, there is a good chance that you are fully protected and will not become infected regardless of the number of contacts." Dr. Longini stresses the importance in distinguishing between the direct and indirect effects of vaccines. A direct effect, Dr. Longini explains, demonstrates how much an individual is protected, whereas an indirect effect shows how much people around that individual are protected. Indirect effects are difficult to measure because the initial vaccination may prevent someone from becoming infected at all, or, if infected, the vaccinated person may transmit infection more poorly. Sometimes direct effects are so great they erase the need for indirect studies. The exploration of vaccine efficacy has taken the researchers to many parts of the globe. In 1991, they analyzed data on a measles outbreak in Burundi to estimate vaccine efficacy. During three months of 1995, Dr. Haber will study at the London School of Hygiene and Tropical Medicine on a Fulbright award. Working with a British research group, which is conducting vaccine research trials in Africa, he will research both design and analysis of vaccine studies. Dr. Longini's work has taken him to Gambia and, most recently, to Bangladesh to study cholera vaccines. In 1993, a massive epidemic of deadly cholera began sweeping across southern Asia. Sponsored by the International Center for Diarrheal Disease Resea rch, an effort is now under way in Bangladesh to conduct a vaccine trial in some 100,000 people, including a vaccine against deadly cholera Bengal. "We are helping design the study to build on our previous experience in vaccine trials," Dr. Longini says. "We have selected sites where high transmission is likely. At least one of the vaccine candidates used in the population will be a live vaccine, such as live oral polio vaccine. Then we will evaluate its direct and indirect effects." The trial, now in Phase I in the United States, should produce findings within the year, enabling researchers to begin the larger trial in Bangladesh. With a five-year award from the NIH, Dr. Halloran studies malarial vaccines. Malaria, transmitted to humans by mosquitoes, kills 1 to 3 million children each year, many of them in Africa. Dr. Halloran recently traveled to Kenya on a site visit to examine the conditions for malaria vaccine firsthand as a member of the World Health Organization/Tropical Disease Research Task Force for Transmission-blocking Malaria Vaccine. The transmissio
n-blocking vaccine is only one of several under study that targets malaria. Another malaria vaccine, called SPf66 and developed by a Colombian physician, reduces the rate of infection by 30% in experimental studies, according to a recent Lancet report. The transmission-blocking vaccine attacks one stage of the disease by producing antibodies in the human host that prevent the malaria stages from forming in the mosquito, thus preventing or reducing transmission.
During the site visit, Dr. Halloran used her knowledge of the biology of malaria and of the statistical methods required for designing a vaccine trial to evaluate conditions for collecting data. Did the site have enough interview personnel? Were they a
ble to produce enough laboratory mosquitoes to do the testing? Would the population cooperate with the study?
The researchers also are exploring vaccine effectiveness in the United States. Dr. Halloran, for example, with investigators from the Centers for Disease Control and Prevention, has studied the effects of routine chickenpox vaccination in preschool chi
ldren, finding that vaccination would substantially reduce the number of hospitalizations. And she has been invited to serve on the Institute of Medicine/National Academy of Sciences Committee on Vaccine Development to help establish vaccine priorities fo
r the United States in the next century.
Dr. Longini spent last summer with NIH researchers conducting Phase I and II trials for an HIV vaccine to ensure it can be used safely. During those trials, the researchers began vaccinating some 1,500 people with a genetically-engineered piece of viru
s to study their immune response. The third phase of trials, currently on hold, will randomly assign vaccine and placebo, with subjects followed over time to determine efficacy.
Researchers are far from the wave of confidence that swept the field when new vaccines for polio, diphtheria, and measles seemed to be preventing some of the most menacing of infectious diseases. Today, more powerful strains of disease are proving resi
stant to all known vaccines and antibiotics. As clinical researchers develop smarter vaccines, they need equally complex tools to test whether their efforts are succeeding. In all likelihood, more researchers will be joining the small band of those with e
xpertise in designing vaccine efficacy studies. For now, Drs. Haber, Halloran, and Longini are contributing their efforts to give a shot in the arm for vaccines. |
 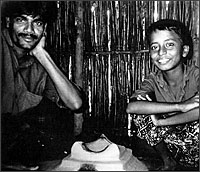 Vaccine efficacy trials take Emory researchers to many parts of the globe, from Washington, DC, to Kenya, from London to Gambia, where these participants in a vaccine efficacy trial recently posed in their home.  In Bangladesh, where this faith healer practices, Dr. Longini is part of an effort to conduct a vaccine trial for some 100,000 people, including a vaccine against the deadly cholera Bengal that is sweeping through the densely populated co untry. |
Spring 1995 Issue | Amazing Grace | 1518 Clifton Road | Economics of the Heart | Back on the Farm
Gunning Down Youth Violence | A Shot in the Arm | Tackling the Sexuality of Teens
Teenaged and Pregnant, Again | Ending Hidden Hunger | Cancer: It All Adds Up
Building Bridges for Reform | Class Notes
WHSC | RSPH
Copyright © Emory University, 1998. All Rights Reserved.
Send comments to
hsnews@emory.edu.
Web version by Jaime Henriquez.