
|
 |
  As special assistant for surveillance at the National Center for Infectious Diseases, Dr. Robert Pinner, 81M, oversees the CDC's response to the growing problem of emerging and re-emerging infectious diseases. |
by Rhonda Mullen Watts
A series of reports in the late 1980s and early 1990s by expert committees convened by the National Academy of Science's Institute of Medicine (IOM) confirmed that the war on infectious diseases was far from over. In fact, according to the reports, the ability of the public health system and health professionals in the United States to deal with emerging infectious diseases was in jeopardy. A variety of factors - human demographics and behavior, technology and industry, economic development and land use, international travel and commerce, microbial adaptation and change, and the breakdown of public health measures - combined to make infectious diseases the major cause of death worldwide. The emergence of new infectious diseases, such as AIDS, and of re-emerging infections once thought to be under control, such as tuberculosis, underscored the severity of the problem. For example, the mysterious hantavirus surfaced in the Southwest in 1993, quickly and fatally striking people who days earlier had been healthy. So many infectious diseases surfaced between 1994 and 1995--with the Ebola virus outbreak in Zaire, a new morbillivirus causing human disease in Australia, and the rapid emergence of antibiotic-resistant bacteria in industrialized nations--that the time became known as the plague year. Publicity surrounding books like The Coming Plague and The Hot Zone and the movie Outbreak pushed the public to near panic. Clearly, something had to be done. |
  "The Georgia Emerging Infections Program has opened many doors for us, giving us direction on how to focus research efforts where they're needed most," says Dr. David Stephens, director of Emory's Division of Infectious Diseases and co-principal investigator of the Georgia EIP. |
A crucial component of this plan is the Emerging Infections Program (EIP), a national network consisting of the CDC and state health departments in collaboration with academic institutions, local health departments, and organizations of health professionals. The network conducts population-based surveillance projects as well as epidemiologic and laboratory projects that address infectious disease threats. It also pilots and evaluates prevention efforts. The CDC initially chose four states to be members of the EIP in 1994: California, Connecticut, Minnesota, and Oregon. Georgia joined the group in 1996, followed by Maryland and New York. In what could be described as a synergistic relationship, Emory's medical school contributes key collaborative expertise to the Georgia EIP, according to Dr. Pinner, who completed a residency in internal medicine here as well as a clinical fellowship in infectious diseases. The school provides research and laboratory resources to the state, augmenting surveillance efforts to track infectious diseases as well as measuring the effectiveness of interventions. An important part of the expertise provided by Emory to Georgia's EIP comes from Drs. Monica Farley and David Stephens, who serve as principal and co-principal investigators for the project. Dr. Stephens, who directs Emory's Department of Medicine's Division of Infectious Diseases, is a noted expert on meningitis and meningococcal disease, while Dr. Farley's major research interest is Hemophilus influenzae. "The Georgia EIP has given the CDC, the state, and Emory a grasp of the prevalence of certain diseases in the Atlanta area," says Dr. Stephens. "It has opened many doors for us, giving us direction on how to focus research efforts where they are needed most." |
  Based on surveillance, infectious disease experts like Monica Farley (standing) know that the incidence of Hemophilus influenzae has fallen dramatically since the introduction of conjugate vaccines between 1988 and 1991. |
Researchers in Dr. Stephens' division, including Dr. Farley's group at the Veterans Affairs Medical Center in Atlanta, have run the Atlanta Metropolitan Active Surveillance program since 1989. This work has now been integrated into Georgia's EIP surveillance, which extends through a 20-county area in which half the state's population resides. EIP surveillance, characterized by "shoe-leather epidemiology," involves direct and regular contact with every hospital and private laboratory in the area to track the incidence of infectious diseases and to collect isolates for testing. Rather than attempting to track all infectious diseases, the EIP targets select pathogens, including Streptococcus pneumoniae, Neisseria meningitidis, group A and group B streptococci, and H. influenzae. EIP surveillance work, both in Georgia and in other states, has been helpful in tracking the relatively new and growing problem of antibiotic resistance, for example. "The EIPs have provided critical information on trends in antibiotic resistance in pneumococcal infections," says Dr. Pinner. Drug-resistant forms of S. pneumoniae have moved from being rare to relatively common in the Atlanta metropolitan area in just a few years. In a report published in the New England Journal of Medicine in 1995, researchers in the Georgia EIP found that one-quarter of 431 Atlanta residents infected with strains of pneumococci had organisms that were resistant to multiple drugs. Some 27% of these isolates were resistant to penicillin - ten times the average rate reported nationwide. Although African-Americans were more likely to be diagnosed with pneumococcal infections than whites, whites were more likely to be infected by a form resistant to drug treatment, says Dr. Farley, one of the co-authors of the paper. In the affluent white suburbs, where residents have easier access to expensive antibiotics, nearly half of the white preschool children with pneumococcal infections were infected with resistant strains, compared with only 17% of African-American children of the same age in the inner city. |
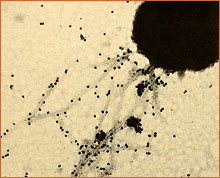
 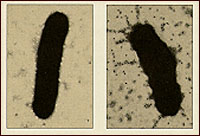 Hemophilus influenzae, formerly the number 1 cause of meningitis in children. The organism at right is piliated, with appendages allowing it to attach to mucous membrane. |
Based on surveillance in Atlanta, for example, researchers Farley and Stephens have reported a dramatic fall in the incidence of H. influenzae disease in children (previously the number 1 cause of meningitis) since the introduction of conjugate vaccines between 1988 and 1991. "The vaccine for H. influenzae has been tremendously successful," Dr. Farley says. "Surveillance not only identifies a problem," Dr. Stephens says, "but also allows us to take that problem back to the laboratory to explore basic science questions." From the surveillance work have spun off laboratory and epidemiological investigations such as those Drs. Stephens and Farley conduct on how organisms function at the molecular level to cause meningitis. For example, in a related project at Emory, Dr. Stephens and others have found that meningococci and other encapsulated microorganisms can escape vaccine-induced or natural protective immunity through a strategy known as capsule switching, in which they change the chemical structure of their outer layer (capsule) of polysaccharide from one serogroup to another. In isolates collected in Oregon and Washington of serogroups B and C, the researchers found that these strains of Neisseria meningitidis were able to convert their capsules from one form to another, allowing them to evade immunity. This finding, published in the Proceedings of the National Academy of Science in 1997, suggests that vaccine prevention strategies should rely on multivalent vaccines that protect against all major capsular serogroups. |
  |
During the past ten years, at least 16 major outbreaks of E. coli O157:H7 have resulted in serious illness and deaths in the United States. Found in undercooked hamburger and roast beef, raw milk, improperly processed apple cider, and contaminated water, E. coli O157 can survive refrigeration and freezer storage. Thorough cooking is the best safeguard against infection. While O157 has been a problem in the Midwest, it occurs less commonly in Georgia, says Dr. Farley. Substantial variation among the EIP sites of the incidence of various foodborne pathogens underscore the need for multi-site surveillance. Both Minnesota and Georgia EIPs are completing case-control studies of O157 as well as Yersinia (the latter contracted during the preparation of chitterlings). The FoodNet component of the EIP seeks to determine the burden of foodborne diseases in this country and the proportion of specific foodborne diseases associated with contaminated food. Its goal is to provide a framework to respond rapidly to emerging foodborne diseases. "The FoodNet helps us gather more specific information about risk factors," Dr. Pinner says. "Ultimately, we want to use this information for prevention strategies." |
  At the Georgia Department of Human Resources, Dr. Paul Blake finds preparedness for controlling infectious diseases to be gradually improving, thanks to efforts such as the EIP. Dr. Blake serves as chief of epidemiology and the DHR's principal investigator for the Georgia EIP. He is assisted by infectious disease epidemiologist, Dr. Jane Koehler. |
"There was concern here that this new variation of CJD might be occurring in this country," Dr. Pinner says. Because of the infrastructure already in place, the EIPs were able to conduct a short-term active surveillance of CJD to look for the new variant. While the study found no evidence of the newly described CJD in the EIP sites, it did demonstrate an ability to gather information rapidly. This flexibility for emergency response is just one of the accomplishments of the EIP network, Dr. Pinner says. "Although there were limitations to the study, we were able to provide preliminary reassurance quickly. The EIP network allowed us an approach that previously was unavailable to us, to pull together this study in a very short time." The field of infectious diseases is "in a better position now than a couple of years ago," Dr. Pinner says. "We're not nearly where we need to be, but we've gotten started." According to Dr. Pinner, some $18 million has been applied to the problem of infectious diseases, but a full implementation of the CDC plan would cost up to $125 million. Dr. Paul Blake, chief of epidemiology in Georgia's Department of Human Resources and the state principal investigator for the EIP, finds the preparedness toward controlling infectious diseases to be gradually improving. "With the additional resources that come from the EIP grant, we're able to put in place a better infrastructure and give more help to the districts." While newspaper headlines continue to announce the appearance of Andromeda-like infections, such as the deadly bullet-proof bug that has turned up recently in six hospitals in Japan, the EIPs' strategy focuses on continuing to build its ramparts through surveillance and laboratory and epidemiological studies. "When it comes to infectious diseases, we're not claiming the sky is falling," Dr. Pinner says. "But we are acknowledging that infectious diseases will continue to pose public health threats. We must avoid complacency to keep ahead of the curve." |
Medicine through the Generations | Great Expectations
The Andromeda Trail | Leaders in the Field | The Next Chapter
Philanthropy News | Events | Alumni News | Class Notes
Copyright © Emory University. All Rights Reserved.
Web version by Jaime Henriquez.