|
 |
 Historically, most of what we know about Alzheimer's has been learned through direct, physical examination of the brains of those who have died of the disease - work conducted by pathologists such as Suzanne Mirra, director of Emory's Alzheimer's Disease Center. |
And that's good. Emory investigators have worked hard with others in the Alzheimer's community to create a template of common goals and approaches to guide research. Bubbling just beneath the surface at Emory, however, is a dynamic program whose energy, vision, and resources mark it as something special. It's a comparatively fledgling effort, led by a multidisciplinary team of young turks who, on occasion, seem to have surprised even themselves with the speed of their progress. Their success rests on an enviable combination of strengths: leadership roles in cooperative ventures sponsored by the National Institute on Aging (NIA); a solid track record of achievement in traditional areas of Alzheimer's research - pathology, radiology, pharmacology; and groundbreaking work in areas such as mitochondrial genetics, dementia in minority populations, and neurodegeneration among aged primates. "A decade ago, neuroscience work at Emory was 150% clinical," says Herbert Karp, founding chairman of the School of Medicine's Department of Neurology. "Today, we can honestly say we have grown fruitful and multiplied." |
 quick look at the landscape of Alzheimer's disease research at Emory won't reveal much that looks all that different from programs in place at our peer institutions.
quick look at the landscape of Alzheimer's disease research at Emory won't reveal much that looks all that different from programs in place at our peer institutions.
 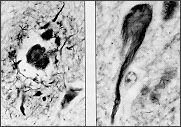 The observation of plaques (left) and tangles at autopsy is still required to make a definite diagnosis of Alzheimer's disease. The recent identification of genetic markers for apolipoprotein E, however, may soon change all that. |
 n a field where growth has been notoriously slow, Emory's rapid rise has not gone unnoticed. n a field where growth has been notoriously slow, Emory's rapid rise has not gone unnoticed.
Since 1907, when German pathologist Alois Alzheimer first characterized the mysterious, progressive dementia which now bears his name, advances in understanding the disorder have seemed incremental, at least to the lay person. There is still no known cause, cure, or treatment; no agreed-upon risk factors; no way to make a definite diagnosis short of autopsy or, in rare cases, biopsy. The principal symptoms described by Dr. Alzheimer - confusion, disorientation, and loss of memory, language, and other higher cognitive functions - are the same chief observational symptoms one sees today. And today one sees more and more of them. Alzheimer's disease is the number one cause of dementia in an increasingly gray USA. More than $90 billion is spent annually on the disease, the NIA estimates, which afflicts almost 4 million Americans and kills about 100,000 each year. If these figures are on target, Alzheimer's should be considered the fourth-leading cause of death among adults in the United States, behind heart disease, cancer, and stroke. Why such glacial progress on such a widespread and devastating illness? Aside from the complexities of the disease, a possible reason is the very nature of academic research itself: insular, highly competitive, and costly. As happens in other disciplines, Alzheimer's researchers have often found themselves in the position of reinventing the wheel, devising their own diagnostic criteria and evaluation methods. In such a breeding ground for diminishing returns, the smallest step forward has required enormous effort. |
 |
 o address the obvious need for pooling of information, the NIA in 1986 created CERAD, the Consortium to Establish a Registry for Alzheimer's Disease. Today, CERAD investigators from 29 university medical centers in this country have joined sites from around the world in collaborative study of Alzheimer's and other dementing disorders. o address the obvious need for pooling of information, the NIA in 1986 created CERAD, the Consortium to Establish a Registry for Alzheimer's Disease. Today, CERAD investigators from 29 university medical centers in this country have joined sites from around the world in collaborative study of Alzheimer's and other dementing disorders.
Emory has long played an active part in this study. At the time CERAD was established, Herbert Karp had just stepped down as chairman of neurology to serve as medical director of the new Wesley Woods Geriatric Hospital at Emory. He eagerly joined forces with the consortium, serving as director of one its first clinical sites. Today, CERAD's neuropathology task force is led by Emory scientist Suzanne Mirra. Other Emory researchers have played key roles in CERAD as well, including radiologist Patricia Davis, who has led the effort to standardize neuroimaging assessments of dementia patients. "I believe our early involvement in CERAD played an important part in coalescing our own research program in Alzheimer's disease," says Dr. Karp, "because it forced us to look around and acknowledge the work that was being conducted here, albeit independently and small of scale. And it set the stage for bigger and better things to take place." |
  Scientists in Dr. John Wood's anatomy and cell biology labs - including Caroline Reich, '94MD, PhD - are looking at enzymes that seem to play a role in affecting tau, a major component of the neurofibrillary tangles seen in Alzheimer's brains. |
he payoff of CERAD's efforts to standardize procedures is that now Alzheimer's researchers can compare apples to apples. CERAD participants, by speaking a common language, are able to stockpile the fruits of their labors into a computerized database for the purposes of comparison and sharing. Dr. Albert Heyman, professor emeritus of neurology at Duke University, heads the consortium, which now follows nearly 2,000 patients in studies around the country. (A widely respected pioneer in neuroscience, Dr. Heyman was a member of Emory's medical house staff in the 1940s and co-founded Grady Hospital's first sexually transmitted disease clinic.)
Emory's connection to CERAD really took off after Dr. Karp introduced Dr. Heyman to Dr. Suzanne Mirra, an up-and-coming neuropathologist. The two hit it off, and it was soon agreed that Dr. Mirra would head up CERAD's new neuropathology task force. "Dr. Mirra quickly became the focal point of our program here as well as a key player in CERAD," says Dr. Karp. "She embraced work from various disciplines - Doug Wallace's research, for instance, on mitochondrial DNA and aging - and really fostered the idea of collective, synergistic work well before an Alzheimer's disease center ever materialized here." One materialized, though, in just five short years, in the fall of 1991. Funded by a $3-million grant from the NIA, Emory's Alzheimer's Disease Center (ADC) is led by Dr. Mirra at the Veterans Affairs Medical Center. "It didn't hurt our grant application to the NIA that we have such a wonderful clinical resource as Wesley Woods or such close ties to Grady Hospital, the Atlanta VA, and the Yerkes Primate Center," says Dr. Karp. "But when it came right down to it, what won us the most points were the people and programs we had in place here at Emory. People and programs have been the core of our success." |
  Mitochondrial genetics expert Doug Wallace is among a growing number of scientists who think Alzheimer's is multifactorial - with genes, environment, and aging all deciding if, when, and how quickly the disease develops. |
n the early 1980s, Dr. Mirra was still devoting most of her time to teaching and clinical practice. One day, she remembers, she was approached by an enterprising first-year medical student, a Woodruff Scholar named John Rogers, who asked for some leads on setting up a summer research project on Alzheimer's disease. She drew a complete blank.
"As inconceivable as it may seem now," she says, "I couldn't think of any basic research going on here in Alzheimer's. But John was tenacious and engaging, and I didn't want to discourage him. So I proposed a project he could do in my own lab." That project, a study of the role of the basal forebrain in neurologic disorders, was published in 1985 in the Annals of Neurology. Dr. Rogers, a 1986 MD/MPH graduate from Emory, went on to a successful neurology career and currently directs the movement disorders program at Beth Israel Hospital in New York. And Dr. Mirra has never stopped proposing projects. One of them, her own, received a merit award on cytoskeletal pathology in 1985 from the VA for work on the physical properties of neurofibrillary tangles and senile plaques in the Alzheimer's brain. That award, now in its third cycle of competitive funding, went a long way toward proving that Emory could play with the big kids on the Alzheimer's playground. Other important research being conducted in the Mirra labs explores the possible connections between Alzheimer's and other neurodegenerative conditions such as Parkinson's and Pick's diseases and progressive supranuclear palsy. "Over the years," says Dr. Mirra, "I have seen an incredible overlap of clinical, neuropathological, and molecular features in these disorders. The microscopic changes that are typical of Parkinson's disease, for instance, are also evident in many Alzheimer's patients." In fact, Dr. Mirra's CERAD group found that about 25% of Alzheimer's cases nationwide show overlapping features of Parkinson's. In a subsequent ongoing study of patients at Emory, Dr. Mirra's ADC team is finding even more overlap. "Approximately one third of our Alzheimer's patients show coexisting neuropathologic features of Parkinson's," she says. "And we've seen that rare conditions like Pick's disease and corticobasal ganglionic degeneration also show a surprising number of shared features. The extent of these overlaps, in fact, suggests these conditions may actually represent a spectrum of disease with related causal mechanisms." The Mirra labs are currently exploring this provocative idea. |
  Molecular geneticist John Shoffner believes Alzheimer's, along with a host of other diseases, may be caused by the progressive depletion of energy in certain cells of the body.
|
 uch of what we know about Alzheimer's disease has been learned through pathology, by scientists such as Dr. Mirra engaged in direct, visual examination of the brains of those who have died of the disease. The two most famous findings - the tangles and plaques that are the microscopic hallmarks of Alzheimer's disease - were first identified at the turn of the century. Much of the work conducted since has centered on unlocking the secrets of these tangles and plaques: Why do they form? What are they composed of? Why do they constitute an apparently benign presence in the brains of some older persons while ravaging the memories and emotions of others? uch of what we know about Alzheimer's disease has been learned through pathology, by scientists such as Dr. Mirra engaged in direct, visual examination of the brains of those who have died of the disease. The two most famous findings - the tangles and plaques that are the microscopic hallmarks of Alzheimer's disease - were first identified at the turn of the century. Much of the work conducted since has centered on unlocking the secrets of these tangles and plaques: Why do they form? What are they composed of? Why do they constitute an apparently benign presence in the brains of some older persons while ravaging the memories and emotions of others?
Much research has focused on the plaques - portions of sick nerve cells mired in a blob of an abnormal protein called beta amyloid. Over the past ten years, literally billions of federal and corporate dollars have been spent trying to crack the beta amyloid riddle - do people with Alzheimer's produce too much of the protein, or break down too little? Further, some researchers dispute just how toxic beta amyloid is to brain cells in the first place, arguing against a direct domino effect linking the protein, plaque formation, and Alzheimer's disease. Emory researchers took a different tack. In the mid 1980s, scientists John Wood, Nancy Pollock, and Suzanne Mirra turned their attention to tangles, specifically to the twisted structures - the paired helical filaments - which are their predominant feature. They determined that a major component of these filaments, which also make up part of the senile plaques, was a protein called tau. In a normally functioning brain, tau is found in axons, the long nerve fibers by which neurons send their electrical signals. In the axons, tau helps fortify the system of microtubules that impart stability to the cell skeleton. One recent study of great interest found that tau binds tightly, in the test tube at least, with apolipoprotein E (ApoE), a protein produced in the liver and brain whose job is to ferry cholesterol around in the bloodstream. One theory has it that one form of ApoE does not bind to tau as it's supposed to, leaving the door open for free-floating tau molecules to clump together, initiating tangle formation and weakening the cell skeleton. Investigators at Duke have found that this "bad" form of ApoE, dubbed epsilon4, is associated with increased risk of developing Alzheimer's. In fact, folks unlucky enough to inherit two copies of e4 (one from each parent) are about 15 times as likely to develop Alzheimer's disease after the age of 65 as are people with none. This link has been confirmed by several groups worldwide, including the Alzheimer's Disease Center at Emory. ADC neuropathologists Marla Gearing and Julie Schneider, working with Dr. Mirra, studied the brains of 100 people with autopsy-confirmed Alzheimer's disease and found that three quarters of them had at least one e4. While Apoe4's identification as a genuine risk factor for the disease is undeniable, says Dr. Mirra, scientists are still leery of calling it the cause of Alzheimer's. "Interestingly, e2s seem to have a protective effect," says Dr. Mirra. "What needs to be sorted out is the actual role, if any, ApoE plays in development of Alzheimer's. One theory has it that ApoE is involved in processing of beta amyloid, which has its own set of implications." ApoE theories, if they pan out, would have to be seen as a boon on the therapeutic front. Instead of having to correct or eliminate a defect in the brain, doctors would be in the preferable position of providing something that isn't there but should be naturally - the protective, binding quality of "good" types of ApoE. But it's not likely to be that simple, Dr. Mirra says. Many people with Alzheimer's disease have no Apoe4; while others with this gene may live into their 90s with no signs of the disease at all. Further demonstrating that ApoE, however important, is not the last piece to the puzzle, Dr. Gearing of the ADC and Johannes Tigges of the Yerkes Regional Primate Research Center at Emory recently published a study of aged chimpanzees identifying the presence of an Apoe4-like gene in the animals. Apoe4, yes . . . neurofibrillary tangles, no. This hallmark of the disease in humans was missing in the elderly chimps, despite the fact that they did have senile plaques and beta amyloid deposits similar to those seen in Alzheimer's. "The ApoE genotype clearly influences the risk of developing Alzheimer's in humans, but we still know very little about how it influences the pathogenesis of the disease," says Dr. Mirra. "My hunch is that while genetic studies will help point the way toward disease mechanism, they will not tell the entire story." |
  "More and more, neuroimaging will play a vital role in the evaluation of dementia," says radiologist Patricia Davis. "It is already an integral part of the examination and follow-up of patients with dementia." |
olecular geneticist Doug Wallace would agree. After years of first establishing then investigating the link between human mitochondria, aging, and disease, Dr. Wallace has come to view Alzheimer's as multifactorial - with genetic, environmental, and aging components all deciding if, when, and how quickly the disease develops. In fact, he thinks a whole host of diseases may be caused by the progressive depletion of energy in certain cells of the body. His theory is tied to OXPHOS, or oxidative phosphorylation, the complex process by which human mitochondria generate ATP, the cellular gasoline that fuels 90% to 95% of the body's activities. OXPHOS, which works chiefly by converting fat to energy, is especially vital for the proper functioning of the brain, heart, liver, and other organ and tissue systems that require very high amounts of energy.
The efficiency with which ATP is generated, says Dr. Wallace, depends on the condition of one's mitochondrial DNA (mtDNA), and that condition is extremely unstable. A maternally inherited form of DNA, mtDNA mutates about ten times faster than the nuclear DNA we inherit from both parents. Even worse, says molecular geneticist John Shoffner, "the mitochondrial mutations themselves can be inherited. The extent of their deleterious impact on ATP production depends, in part, on the severity of the mutations and their location within specific cells of particular organs." Furthermore, we acquire even more mutations to our mtDNA as we age, and the accumulated damage eventually slows down ATP production to the point where there is simply not enough gas left to keep the engine running. Without ATP, cells shut down and die. Enough dead cells in any one organ or tissue system and it malfunctions. Alzheimer's disease - characterized by the progressive death of specific brain cells and with demonstrated risk factors linked to age, environment, and inheritance - may have a mitochondrial OXPHOS connection. Speculative at this point, Dr. Wallace admits, but intriguing. He is willing to bet that OXPHOS-connected defects will hold answers not only to the cause of Alzheimer's and other neurodegenerative disorders but to other age-related conditions, including heart disease, cancer, and diabetes. |
 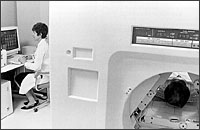 "The 'functional' images generated by PET and SPECT afford us rare glimpses into the inner workings of the human brain," says radiologist Naomi Alazraki, clinical director of PET imaging at Emory Hospital. Emory's PET center is one of only 60 in the nation. |
he problem with an inability to metabolize something, of course, is that typically one doesn't know it until it's too late. That's certainly true of a disease marked by progressive metabolic dysfunction. By the time the average patient is brought to a doctor with full-blown clinical symptoms of Alzheimer's, for example, as much as 80% of some regions of his or her brain may be irreversibly degenerated. Therapy, even if it existed, could do precious little at that point.
But some Emory radiologists are hopeful that advances in nuclear imaging - particularly in positron emission tomography (PET) and single photon emission tomography (SPECT) - can help brighten that grim picture. "The images generated by PET and SPECT are what we call 'functional' images, to distinguish them from the anatomic images provided by x-rays and magnetic resonance imaging (MRI)," says Naomi Alazraki, co-director of nuclear medicine and clinical director of PET imaging at Emory University Hospital. "They require living, functioning cells, and by looking at them we can see metabolism, perfusion, blood flow - the stuff of life. They afford us rare glimpses into the inner workings of the human brain." For instance, says radiologist Patricia Davis, PET specialists can now visually track the metabolism of glucose and oxygen in the brain, which is known to be abnormal in a person with Alzheimer's disease. The merging of such metabolic imaging tools with the superior structural abilities of MRI holds much promise, says Dr. Davis, for the early diagnosis of Alzheimer's as well as for the monitoring of potential therapies. What's needed to make this possible, she says, are large-scale studies on patients with different forms of dementia, as well as on healthy aged people with no dementia. "That is why collaborative projects such as CERAD are so important. It's the only way we can ever hope to see the sheer numbers of brains we need to further our knowledge." CERAD's registry of people with probable Alzheimer's is also important, says Dr. Davis, should the day come that a meaningful therapy is developed. "At that point, the national registry could aid in identifying people who could benefit from clinical trials." Another, more proactive scenario could be imagined for the not-too-distant future: A person known to be at increased risk for Alzheimer's disease - because of family history, for example - might start having brain scans at a certain age to detect the advent of the disease. Physicians could then search for early signs of Alzheimer's - degeneration in the medial temporal lobes, incomplete metabolism in the basal forebrain - much as they search today for the radiologic shadows and spots that presage breast cancer. Unfortunately, given current technology, functional brain imaging, particularly PET, is a labor-intensive, prohibitively expensive, and complex technique, especially in patients with a limited capacity to cooperate with a procedure that can last as long as an hour and a half. Availability is another limiting factor; only 60 PET centers exist in the United States, and all are in academic research settings. But there is little doubt, say Drs. Davis and Alazraki, that functional brain imaging can provide useful information in research studies and that the lessons learned in the lab will one day be extended to the bedside. |
  Overlapping causes of dementia are particularly prevalent in African-Americans, says neurologist Alex Auchus. While Alzheimer's disease is the most common, other culprits include vascular disease, diabetes, and nutritional deficiencies. |
 hen all is said and done, when all tangles have been tallied and all plaques accounted for, Alzheimer's disease remains a stubbornly behavioral problem. No one sends their loved one to a nursing home because of dots and spots on a pathologist's slide. hen all is said and done, when all tangles have been tallied and all plaques accounted for, Alzheimer's disease remains a stubbornly behavioral problem. No one sends their loved one to a nursing home because of dots and spots on a pathologist's slide.
"The troublesome behavior that Alzheimer's patients exhibit is often more significant in having them sent to nursing homes than their cognitive decline," says neurologist Alexander Auchus, head of the ADC's satellite clinic at the DeKalb-Grady Neighborhood Health Center. "Even if a patient has a bad memory, if he is able to sleep at night and cooperate with caregiving, he is much more likely to stay at home than is a patient with a better memory but who refuses to bathe and change clothes, or who is up at night walking around the house." Fortunately, he says, the sleep disturbances, anxiety, agitation, and other secondary behavioral symptoms of Alzheimer's disease often respond to treatment, either with medications or with certain nonpharmacologic approaches. What complicates matters is that a fair number of people who go to their doctor complaining of memory loss actually have more than one cause for the problem, and those separate causes must also be diagnosed and treated, which can be a complicated process. "A given patient may be found to have Alzheimer's by clinical criteria," Dr. Auchus says, "but when we check his or her blood we may find a vitamin B-12 deficiency, which can also cause dementia. Or perhaps we'll find strokes or depression coexisting with the Alzheimer's disease. These are all common problems in an elderly population." He has found overlapping causes of dementia to be especially prevalent in the predominantly minority population seen at the DeKalb-Grady Clinic. In a recent study, he and his colleagues found that about half of the African-American patients at their clinic who were demented had what could be termed "pure Alzheimer's disease"; 16% had overlapping Alzheimer's and vascular dementia, and 34% had multiple causes, including nutritional deficiencies and alcoholism. "These findings fly in the face of the popular misconception that strokes are the major causes of dementia in black Americans," says Dr. Auchus. "There has always been a sort of apocryphal wisdom, even among doctors, that Alzheimer's is a white, middle class disease. Perhaps cultural and financial concerns have prevented black families from seeking medical or institutional care for their loved one with dementia, and they have therefore been statistically under-represented. Nevertheless, our studies show that in Atlanta, at least, Alzheimer's is the most common cause of dementia in blacks, just as it is in whites." |
  In advanced Alzheimer's, the brain is no longer able to produce sufficient quantities of the neurochemicals acetylcholine, serotonin, and glutamate, which are essential to proper brain functioning. Using the Parkinson's/dopamine model, neurologist Allan Levey and others at Emory are working to develop drugs to replace these missing chemicals.  "The fact that we still don't have a biological test for Alzheimer's is a major stumbling block," says Dr. Charles Nemeroff, chair of Psychiatry and Behavioral Sciences. "We would like to develop one - using spinal fluid, blood, urine, or some other peripheral tissue - with which we could make a diagnosis." |
mplicit in the wide scope of Alzheimer's investigations being carried on at Emory and elsewhere is the general issue of the heterogeneity of the disease. There is no one-size-fits-all definition of Alzheimer's; rather, each case comes with its own particular set of clinical symptoms, its own timetable for progression, its own pathophysiologic thumbprint. And although this throws the door wide open for many areas of research, says Dr. Mirra, the downside is that science will not arrive easily at a single cause, diagnostic test, or treatment.
"I wouldn't hold my breath for it," she says. "But even if a therapy cannot prevent or cure the disease completely, one shouldn't ignore the tremendous importance of merely delaying disease progression. Just by postponing institutionalization, patients and their families could realize enormous emotional and financial savings." That must have been the spirit in which the FDA approved its first-ever Alzheimer's drug this past September. That drug, tacrine, works by slowing the breakdown of acetylcholine, one of several essential neurochemical transmitters that become deficient in the Alzheimer's brain. Since its widely publicized release, however, tacrine has been greeted largely with a chorus of yawns from the medical community, showing only limited therapeutic benefits and some severe side effects, particularly liver damage in about 20% of patients taking it. "If tacrine were another drug in a larger cast of characters, so to speak, it probably wouldn't have been approved," says Charles Nemeroff, chairman of Psychiatry and Behavioral Sciences at Emory. "But as the only one, it is viewed as the lesser of two evils, sort of like the AZT of Alzheimer's disease." In the limited number of people who can tolerate it, tacrine sets the clock back on the advance of Alzheimer's disease by about six months, according to neurologist Allan Levey. "After that, the disease continues to march forward. Much like Parkinson's therapy with dopamine, tacrine merely offsets some of the symptoms of the disease but doesn't do anything to halt its progression." The problem, says Dr. Levey, is that Alzheimer's is a much more complex disease than Parkinson's. "Although acetylcholine deficiency is the most prominent deficit in the Alzheimer's brain, several other neurotransmitter systems also degenerate consistently: for instance, serotonin and glutamate, both of which are absolutely critical for proper cognitive functioning." Dr. Levey currently is studying receptors for these various neurotransmitters in both animal and human brains in hopes of clarifying how they might be relevant in development of more specific and effective drugs. Despite tacrine's limitations, Dr. Levey says, it is still an encouraging advance in drug therapy against Alzheimer's. "The point is that tacrine, simply by enhancing the action of just one of the three major chemicals that are deficient, has shown some benefit in seven of ten people who can tolerate high doses of the drug. And it's important to remember that the people taking tacrine are typically in the middle stages of Alzheimer's, not the early stages. So it's remarkable, when you consider they have already suffered substantial brain damage, that they are actually experiencing any positive effect." * * * Keeping in mind the benefits of each tiny scientific step forward can be a challenge to those who struggle daily with the less theoretical aspects of Alzheimer's: the families and caregivers of those with the disease. It's a lesson Sue Mirra learned the hard way. "I was already very involved in the field as a researcher when my father developed Alzheimer's. He died several years later, at the age of 86. The problems my mother, my brother, and I faced caring and making decisions for him during those years really opened my eyes. It made me more sensitive to the needs of caregivers." It's an experience she thinks is worth sharing. Eight years ago, with that thought in mind, she initiated a program with the Atlanta chapter of the Alzheimer's Association that brings second-year medical students in contact with families of Alzheimer's patients. The students visit patients and talk with their family members about the emotional, physical, and financial stresses they face. Not only has the program been an unqualified success among students, several families sign up year after year to participate. "It's an easy, practical way to teach our future physicians that there's more to disease than plaques and tangles," says Dr. Mirra. "There are people involved." |
Mechanics of the Mind: Unlocking the Mysteries of Alzheimer's Disease
Insights into Cancer: Exploring Cell Biology
Humanizing Medical Education | Alumnus Profile: Off the Beaten Path
Copyright © Emory University. All Rights Reserved..
Web version by Jaime Henriquez.