 | 
|
On the one hand, researchers and caregivers alike are faced with increased competition for dwindling dollars, less say in how those resources are allocated, and mounting political pressure to manage costs at any cost. On the other hand is a clear and present danger. More than 14 million people worldwide are thought to be infected with HIV. In this country, more than 200,000 people have died of AIDS in the past 13 years, and 150,000 more are expected to die in just the next 14 months. In Georgia, enough men, women, and children have AIDS to rank this state 11th in the nation; among cities, Atlanta is seventh. The School of Medicine at Emory - based on the strength of its faculty, research, clinical sites, and partnerships on campus and in the community - is in the enviable position of being able to respond to AIDS as extensively in the laboratory as at the bedside. Not only is the school consistently competitive for federal and foundation grants, but it is also able to translate funds into exciting new therapies and compassionate care for the thousands of Georgians with HIV and AIDS. It didn't happen overnight, and much work is still in progress, but as attested by a spate of recent awards, openings, and initiatives, Emory has put together a solid foundation from which to wage a meaningful war against AIDS. |
 Dr. Sumner Thompson has spearheaded Emory's clinical work in AIDS for the past seven years. |
 he single largest source of care for HIV-positive Georgians is the infectious disease clinic (IDC) run by Emory doctors and Grady Memorial Hospital nurses and physician assistants. The IDC, which served just a couple of hundred patients when it opened at Grady in 1986, now ministers to roughly 4,500 people. Projections have the clinic growing at an annual rate of 10% to 12% for each of the next five years, making it the fastest-growing component of the Grady Health System. This bleak picture was made brighter by the opening this past October of the new Ponce de Leon Center, a facility in Midtown Atlanta that joins under one roof the IDC and all the auxiliary AIDS programs created at Grady over the past eight years.
The center is directed by Dr. Sumner Thompson, who was recruited to the full-time faculty in 1987 to head up the medical school's AIDS efforts. "In those days, the IDC at Grady had just gotten off the ground," he says. "It was an opportunity for me to work in an area that needed me." he single largest source of care for HIV-positive Georgians is the infectious disease clinic (IDC) run by Emory doctors and Grady Memorial Hospital nurses and physician assistants. The IDC, which served just a couple of hundred patients when it opened at Grady in 1986, now ministers to roughly 4,500 people. Projections have the clinic growing at an annual rate of 10% to 12% for each of the next five years, making it the fastest-growing component of the Grady Health System. This bleak picture was made brighter by the opening this past October of the new Ponce de Leon Center, a facility in Midtown Atlanta that joins under one roof the IDC and all the auxiliary AIDS programs created at Grady over the past eight years.
The center is directed by Dr. Sumner Thompson, who was recruited to the full-time faculty in 1987 to head up the medical school's AIDS efforts. "In those days, the IDC at Grady had just gotten off the ground," he says. "It was an opportunity for me to work in an area that needed me."
The extent of that need became even more apparent as the clinic outgrew three sites in six years. "This time around, we looked long and hard for a property that could expand to meet our needs," says Dr. Thompson. "The new building has about 40,000 square feet with expansion capabilities for another 10,000. I would go so far as to say that what we have now is the state-of-the-art clinical program in the country." Beyond size, however, what sets the Ponce de Leon Center apart is the range of services offered on site. A women's clinic, for example, serves a population that now comprises 18% of Grady's AIDS patients. It is augmented by a family clinic that offers simultaneous treatment of HIV-infected women and their children, which links in turn with a pediatric AIDS clinic. Directed by pediatrician Steven Nesheim, this clinic follows more than 60% of the state's pediatric AIDS case load. Dr. Nesheim directs six NIH pediatric AIDS clinical trials at the center, with three more to be added soon and plans being laid for an adolescent group. Additionally, the IDC supports a preventive and restorative dental program, headed by Dr. David Resnik; a full-service pharmacy; and an adult mental health program, run by Dr. Stephen McDaniel, that will expand in April to include pediatric mental health services. The center also works closely with the Emory AIDS Training Network to provide education and training to health care professionals throughout the state. The IDC has an active research program as well, according to Dr. Thompson, both in the treatment and epidemiology of HIV disease. The IDC recently received $5 million from the US Centers for Disease Control and Prevention to support tuberculosis research that will link with ongoing IDC-directed AIDS investigations. "In addition, we are currently running more than 20 research protocols," says Dr. Thompson, on such things as combination antiretroviral therapy, fluconazole treatment of esophageal ulcers, and studies of mycobacterial infections. The latter is an area in which the IDC has gained a national reputation. Managing the myriad opportunistic infectious of the HIV-positive patient is a daunting task, but one where results can be readily seen. "There is no question that our HIV-positive patients are living much longer and are capable of carrying on independent lives for much longer," Dr. Thompson says. "This has a lot to do with the drugs we give them, of course, but also with the support they get from our whole range of programs. We provide job retraining, for instance, for those who can no longer do the job they used to do. I consider this an integral part of primary care for an AIDS patient. Ultimately, being able to provide a totality of care is our final goal." |
  Dr. Sharne Sheehey practices at the women's AIDS clinic in the new Ponce de Leon Center. A letter she wrote to Mother Teresa about the plight of Atlanta's homeless AIDS population led to the opening this past November of a hospice in Midtown for HIV-infected mothers and their children. Nuns from Mother Teresa's order will provide food and shelter for the residents. Staff from the Ponce de Leon Center will provide health care. |
 mory's ability to meet this goal has been enhanced on several fronts in some very practical ways. One of these is the ongoing clinical work being done by Emory retina specialist Dan Martin. mory's ability to meet this goal has been enhanced on several fronts in some very practical ways. One of these is the ongoing clinical work being done by Emory retina specialist Dan Martin.
When Dr. Martin, a former chief resident in ophthalmology at Emory, returned here in September 1993 after finishing an ocular immunology fellowship at the National Eye Institute, he was involved in an NEI Phase I clinical trial aimed at halting the progression of cytomegalovirus retinitis, the most common cause of blindness in people with AIDS. The conventional therapy for CMV retinitis - ganciclovir or foscarnet infused daily through a chest port - is costly, time-consuming, and labor intensive for both patient and physician; even worse, the disease usually continues to progress anyway. Further complicating the situation is the very nature of a fixed catheter, which may get infected and often causes psychological and logistical hardships for the patient. In the trial, Dr. Martin is testing a drug delivery system developed by researchers at the University of Kentucky that involves surgically implanting a pellet in the eye, which, over several months, releases small, regular doses of ganciclovir directly into the vitreous cavity. Dr. Martin has performed about 40 of these implants, and results have been very encouraging. In a new study, Dr. Martin plans to begin recruiting local patients early this year for a large-scale clinical study of the ocular implant used in conjunction with oral doses of ganciclovir. "Because CMV is a systemic infection," he says, "our concern is that local treatment won't offer much protection to the other organs in the body which can be affected by the virus." The implant, then, will get the drug quickly to the area most often affected by CMV, the eyes, while the oral dose will combat system-wide infection. Dr. Martin's work at Emory over the past six months has been conducted largely without the benefit of formal laboratory space, a situation which will be rectified, in part, with federal funds received this past November. A new NIH/NEI construction grant, the first awarded in the state in the past decade, will partially support the completion of two unfinished floors at Emory's South Clinics as well as the outfitting of 7,100 square feet of lab space to be dedicated to Emory Eye Center investigators, including Dr. Martin. The grant, directed by School of Medicine Dean Jeffrey L. Houpt and ophthalmology researcher Henry F. Edelhauser, was the highest-ranked eye study proposal funded by the agency. Other labs planned for the space will be used by research programs in AIDS, cancer, transplantation immunology/autoimmunity, and molecular and human genetics. |
  Dr. Dan Martin, a new faculty member in ophthalmology, will soon recruit patients for a large-scale clinical trial of an ocular implant used to prevent AIDS-related blindness. |
|
ven more far-reaching in its scope and collaborative nature is the Research Center on AIDS and HIV Infection (RCAHI), which will be housed at the Atlanta Veterans Affairs Medical Center adjacent to campus. As announced this past October, School of Medicine faculty have competed for and won a five-year, $2.5-million grant from the VA to establish this comprehensive AIDS research center, one of only four sites in the nation to win these federal funds. Of the 11 applications selected for peer review, Emory's proposal was ranked first.
Dr. David Rimland, in the Department of Medicine's Division of Infectious Diseases, supervises all HIV-related work at the Atlanta VA, including an AIDS program already in place there that follows approximately 550 patients. He will serve as director of the RCAHI and of its clinical staff, as they look at problems with drug resistance, conduct pulmonary research and epidemiological studies, and follow the pathogenesis of many HIV-related opportunistic infections. The scientific director of the RCAHI is Emory professor Raymond Schinazi, an internationally prominent antiviral drug researcher who will lead the basic research team in the areas of virology, pharmacology, and opportunistic infections. In all, 15 Emory investigators will work at the new research center. They will have a lot of help. Scientists from the University of Georgia, Georgia State University, and the CDC, many of whom already work with Emory researchers on other AIDS-related projects, will join forces in the venture, contributing primarily to basic research. The clinical area will get support from the AIDS Research Consortium of Atlanta (ARCA) - an affiliation of 47 physicians in private practice and at the infectious disease clinics at Grady, the VA, and Southside Health Care. ARCA, a primary source of clinical AIDS trials in Atlanta, monitors thousands of HIV-infected patients and will provide a vital clinical outlet for the RCAHI's basic science. Hopes are high for the new center. "We think this much-needed infusion of funds - together with the partnership of our fellow academic researchers and community-based clinicians - will foster a cohesion of effort," says Dr. Schinazi. "We hope it will lead to truly great things." |
  Antiviral drug researcher Raymond Schinazi thinks HIV will one day be controllable through a combination of chemotherapies. "We don't need to look only for home-run cures for AIDS," he says. "I am happy to get to second or third base to find ways to prolong the lives of patients." |
|
he Schinazi labs are as likely a place as any for important advances to emerge, particularly in the arena of antiretroviral drugs. He holds patents on 11 drugs designed to inhibit viral activity, three of which are currently in clinical trials. A score more are in the pipelines.
He hopes one or more of these will prove safe and effective in lulling the virus into a constant state of latency, transforming it into something akin to a sleeping viper the infected person can co-exist with, albeit uneasily. With diligent medical management, he believes, we might be able to learn to live with that which threatens to kill us. "Because of latency, I don't think we'll ever be able to totally eradicate HIV from a person," Dr. Schinazi says. "But we can try to prevent its reactivation." As with the herpesvirus, he explains, HIV retreats into a long period of dormancy following the initial period of infection. "We don't know what makes the virus express itself, what triggers it to move from a dormant stage to an active one. If we can solve this enigma, we should be able to develop drugs that can prevent the virus from reactivating and put the cells that are already activated into permanent latency." |
 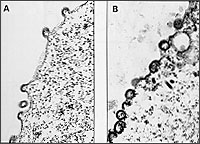 Bad expression: The nodules on the edge of this HIV-infected cell are the first physical evidence that the virus is beginning to be expressed (A). In the later stages of infection, the nodules create a chain link fence-like effect around the periphery of the cell (B). When the cell dies, the virus will discard it and seek another host for replication. |
 hile the attack on AIDS being mounted by Dr. Schinazi and other Emory researchers is essentially a therapeutic one - with the goal of extending and ultimately saving the lives of people already infected with HIV - a scientist on the other side of campus, at the Rollins Research Center, is trying to prevent infections from taking place at all. hile the attack on AIDS being mounted by Dr. Schinazi and other Emory researchers is essentially a therapeutic one - with the goal of extending and ultimately saving the lives of people already infected with HIV - a scientist on the other side of campus, at the Rollins Research Center, is trying to prevent infections from taking place at all.
Dr. Richard Compans, one of the world's pre-eminent research virologists, was recruited to Emory in 1992 to chair the Department of Microbiology and Immunology. He is leading a National Cooperative Vaccine Development Group, funded by the NIH, that is working on a vaccine to protect against sexual transmission of HIV. It is the missing link in vaccine development; to date, he says, none of the 15 or so AIDS vaccines undergoing clinical testing offers such protection, even though three fourths of all HIV transmissions are, in fact, sexual, not blood-borne. Nevertheless, most HIV vaccines are blood-borne, he says, because they are designed to be injected - emulating tried-and-true models like the shot for influenza. Such an approach stimulates serum rather than mucosal immunity and offers little protection when the initial viral contact is made at the genital-mucosal membrane, as is typically the case when HIV is transmitted sexually. Dr. Compans' group has developed a two-part vaccine - one part injected but the other taken orally to stimulate the mucosal immune system. The combination has shown remarkable success in protecting rhesus macaques against vaginal infection by the simian immunodeficiency virus (SIV). Such vaccine protection had never been demonstrated before, he says. In terms of eventual application to human AIDS, though, a few wrinkles are still being ironed out in the lab. First, the macaque vaccine was made from live, infectious SIV inactivated with formalin, an approach which is undesirable in human trials. Dr. Compans' team has sidestepped this problem by developing a genetically engineered, or recombinant, model that has some of the same structural parts as HIV but lacks the nucleic acids needed for viral activity. To get the orally administered vaccine safely past the stomach's acids, the researchers have devised a method of embedding the recombinant antigen in biodegradable polymer spheres. Once these are safely through the digestive system, they are taken up by the cells of the immune system, where the polymer breaks down and releases the vaccine components. Based on the promising results seen so far, the NIH has re-funded Dr. Compans' simian vaccine project for another four years. In the second leg of the study, he and his collaborators plan to work with a larger group of animals and address a new set of questions: By what mechanism does the vaccine prevent infection? Will the immune response work against different strains of the virus? How long will the immune response last? |
  Dr. Richard Compans, one of the world's leading research virologists, is working on a vaccine to prevent sexual transmission of HIV. |
 f the world of AIDS research sometimes seems split into the black-and-white camps of prevention and therapy, it's not because it has to be that way. In fact, Emory immunologist Aftab Ansari thinks combining the two approaches - by introducing antiretrovirals into a revved-up immune system - might get better results than either does alone. f the world of AIDS research sometimes seems split into the black-and-white camps of prevention and therapy, it's not because it has to be that way. In fact, Emory immunologist Aftab Ansari thinks combining the two approaches - by introducing antiretrovirals into a revved-up immune system - might get better results than either does alone.
"Because chemotherapy, in general, inhibits viral replication regardless of the strain, it is very useful in controlling virus load," he says. "Chemotherapy, in tandem with a vaccine broad-based enough to induce a strong humoral and cellular immunity, could very well produce the one-two punch we need to stop this virus." In 1985, when Dr. Ansari came here from the NIH, his reputation was primarily in autoimmunity and transplantation. However, an important discovery at the Yerkes Regional Primate Research Center at Emory helped turn his attention to AIDS. Scientists there in 1985 had found that their colony of West African sooty mangabeys was naturally infected with SIV and that the virus, when isolated and injected into rhesus macaques, caused the onset in the macaques of an illness very similar to human AIDS. "At the time, they were studying the progression of disease in the macaques," says Dr. Ansari, "but I was intrigued with the fact that the infected sooty mangabeys remained completely healthy. It is a very interesting model, one that made me wonder what mechanisms are involved in the protection of mangabeys and the susceptibility of macaques to what is supposedly the same virus." "The sooty mangabey has developed a population of cells that appears to regulate virus replication so the amount of virus remains very low," he continues, "and in the presence of this low virus load it is possible that the immune system that develops is quite different from the other species', in which virus replicates to very high levels." If he can determine the molecular mechanism by which these regulatory cells work, it could possibly be used in a vaccine aimed at keeping virus presence minimal. "An insidious aspect of HIV is that it replicates within the very immune cells that are supposed to fight it," says Dr. Ansari. "It might be our immune response against the virus that eventually destroys us. Perhaps we shouldn't even try to induce a protective response. It's not necessarily going to be protective to create more and more of the cells which the virus invades, replicates within, and kills. We may have to learn how to educate our immune system not to recognize the virus as foreign and how to selectively induce low virus replication. Maybe then we can live with HIV happily ever after. Perhaps this is what the sooty mangabey has done." Working with Yerkes puts Dr. Ansari in a unique position to find an answer. The primate center has the country's only research and breeding colony of sooty mangabeys and has developed the world's only series of reagents and assays specifically geared to study the immune responses of rhesus macaques. This extensive baseline work and one-of-a-kind investigative potential was recognized in 1988 with a five-year NIH grant, which Dr. Ansari submitted for renewal this past fall. |
  Immunologist Aftab Ansari thinks we can try to teach the immune system not to recognize HIV as foreign. Maybe then, he says, we can live with HIV, much in the same way that the sooty mangabey monkey co-exists with simian immunodeficiency virus.  The sooty mangabey's ability to remain healthy despite infection with an AIDS-like virus is of enormous interest to those seeking ways to save the lives of people infected with HIV. The Yerkes Regional Primate Research Center at Emory has the nation's only research and breeding colony of these primates. |
 IDS researchers, at Emory and elsewhere, may disagree on the details of how their work should be done, but they all acknowledge its urgency. That urgency, articulated by AIDS activists and by many members of the medical community, led the Food and Drug Administration a few years back to create a special fast-track approval process for AIDS-related therapies that speeds the fruits of research to those who need them most. The mechanism of testing these therapies, of course, is the clinical trial. IDS researchers, at Emory and elsewhere, may disagree on the details of how their work should be done, but they all acknowledge its urgency. That urgency, articulated by AIDS activists and by many members of the medical community, led the Food and Drug Administration a few years back to create a special fast-track approval process for AIDS-related therapies that speeds the fruits of research to those who need them most. The mechanism of testing these therapies, of course, is the clinical trial.
The School of Medicine presently supports an active slate of AIDS trials, for both adults and children, says Dean Jeffrey L. Houpt. "Faculty in the Division of Infectious Diseases alone, for example, are conducting about 25 clinical AIDS studies and about 30 epidemiological and psychosocial research projects." But the school is committed to further expanding its clinical AIDS profile, he adds, and to that end is busy assembling the requisite resources and documentation to apply for an adult AIDS Clinical Trial Group designation from the NIH. Dr. David Stephens, director of Infectious Diseases in the Department of Medicine, is the point man as Emory prepares to make its application for the federal funds, to be awarded during the NIH's 1995 grant cycle. Such a site in Atlanta, he says, would allow literally thousands of Georgians to take advantage of new AIDS therapies years earlier than otherwise possible. "Right now, we're focused on building a foundation for success for the ACTG application by reinforcing our clinical and research programs," says Dr. Stephens. "We're presently interviewing for several new faculty positions at Grady and the VA, and we're also shoring up our nursing and support staff. We want to be able to hit the ground running." "In preparing what we hope will be a successful application, we have a number of points in our favor," he says. "We've built deep, reciprocal ties on a variety of community levels. The new facility on Ponce de Leon, where the ACTG effort would likely be centered, is in itself a major advantage. Our infrastructure is strong, and our faculty is strong and getting stronger." "But perhaps the greatest case to be made for an Emory ACTG is the sheer number of patients who could enroll in clinical trials as a result. For purposes of data collection, this represents a statistical gold mine. For those of us involved in the daily care of sick and dying patients, it represents a golden opportunity to provide the latest in therapy. It's a chance we don't want to miss." |
  Infectious disease specialist David Stephens is preparing Emory's application for federal funds that could allow thousands of Georgians to take advantage of new AIDS therapies. |
Life Under the Sickle | The Shape of Things To Come
Inside a Private World | A Leader in Good Time
Copyright © Emory University. All Rights Reserved.
Web version by Jaime Henriquez.